Interest in the Buteyko method has picked up recently. Many common misconceptions I spent years trying to dispel have also resurfaced. I find myself writing the same answers to the same questions over and over again, while new people engage with false and outright predatory information online.
I decided to sit down and write a rough first draft with the very basics of the theory of the Buteyko method, as well as a FAQ section, so I have a post to link when someone comes looking for answers.
Subscribe or Perish
This isn’t an exhaustive list, by no means, but I’ll try my best to give you a comprehensive overview.
I won’t provide research links just yet.
I’m not willing to argue the efficacy of the method here - it’s pure information in regards to what Dr. Buteyko and I believe, whether you agree or not.
I won’t try to avoid jargon.
At the end of this article, you’ll find a couple of simple exercises.
This isn’t medical advice - use common sense.
Ask questions and I might include them in the FAQ section.
If you’re here just for the practical stuff, read #1, #2, #3, #4, #7, #12, #13.
Bookmark the page because I’ll keep adding and expanding as I see fit.
Let’s begin.
1) Brief Biography (a)
Dr. Buteyko was a scientist and doctor in the 1950s who noticed he could prevent an angina attack by slowing down his breathing. His symptoms, on the other hand, became worse when he hyperventilated (rapid breathing)
Eventually, he noticed a similar pattern in his patients. He believed that “hyperventilation at rest” was the culprit to most of modern man’s ailments, becoming their cause, as well as the symptom, and creating a positive feedback loop. He was able to conceptualize a method that eliminated their symptoms and addressed the root cause.
(One example of this feedback loop can be observed in the “Hyperventilation Provocation Test” used clinically to assess weak links in the organism)
The Buteyko method is now known for its efficacy in treating asthma, but according to Dr Konstantin and his colleagues, they were able to treat multiple illnesses during their clinical trials.
2) Voluntary Elimination of Deep Breathing Method (b)
That’s the name of the original method and was based on simple relaxation breathwork techniques that stopped hyperventilation on its tracks.
He shared his ideas openly but was met with derision. There’s a rumor that he prepared fliers with instructions and threw them around in the streets of Novosibirsk out of desperation.
Eventually, the method evolved and he was able to test it in 1,000+ asthma and heart patients during the 1960s, and in most of Europe, eventually getting accepted as a valid supplementary treatment method by the Russian Federation of Health.
Dr Buteyko went on to participate in other research, but given he contributed to the Soviet space program makes his steps hard to track. We know from a declassified CIA memo that he was involved in ESP research, with agents describing that he had “perfected his method”, which included transmission of bioenergy… but that doesn’t tell us anything concrete.
He continued to advocate for his method, teaching and healing throughout Europe, including royalty like King Charles. He founded institutes that continue propagating his techniques to this day. Dr Buteyko died in 2003.
3) What’s NOT the Buteyko method
I’m always surprised by how difficult it is to find a specific and simple definition of the method or an exercise that actually adheres to what Buteyko is supposed to accomplish.
For that reason, we tend to fill our knowledge gaps by borrowing information from other, familiar contexts:
It’s not pranayama.
It’s not box breathing, 4-7-8, or slow nose breathing.
It’s not breath holds or Wim Hof.
It’s not about increasing your VO2max.
It’s not freediving style of breath holds.
It is NOT just the Control Pause test (see #7)
It isn’t about forcefully breathing in a particular way. It’s not a technique that you need to practice 24/7, but it’s also not a drive-through method you can do for a couple of months and be done with it.
Buteyko isn’t about becoming more relaxed in the moment, alleviating anxiety, or just feeling better for a few hours. It’s not one technique, a system.
4) The Buteyko Method
Let’s attempt a practical definition:
It’s reducing the tidal volume of respiration until the sensation of air hunger arises, and then maintaining that uncomfortable sensation for 15-40 minutes, while staying relaxed. This is why different breathing exercises fit the bill.
It’s about changing your reflexive, unconscious, 24/7 breathing pattern.
It’s about transforming how you’re breathing on a biochemical and neurological level.
It’s about increasing the generation of energy in the cells.
It’s about lasting changes that stay beyond the end of a session.
It’s about raising your baseline energy levels, riding the upward spiral of metabolic adaptations.
Buteyko has a rich theory and a complicated mechanism of action that begins with carbon dioxide and how it behaves within the body but extends to the very function of your cells and neurons.
For the exercises, see #11 but they’ll make more sense if you understand the basic theory that we’ll discuss right now.
5) Carbon Dioxide
At this point, it’ll be useful to give you more context about CO2.
There’s a misconception, perpetuated by an incomplete understanding of biochemistry, that carbon dioxide is simply the “waste gas” of cellular respiration.
This is a term still being used, with all of the negative connotations it carries after Antoine Lavoisier used it in the context of his oxygen theory of combustion in 1774.
In recent years, we’ve understood the major role CO2 plays in every metabolic pathway of our physiology.
And while it’s true that it is a by-product of cellular respiration, it is very much responsible for the oxygenation of our cells.
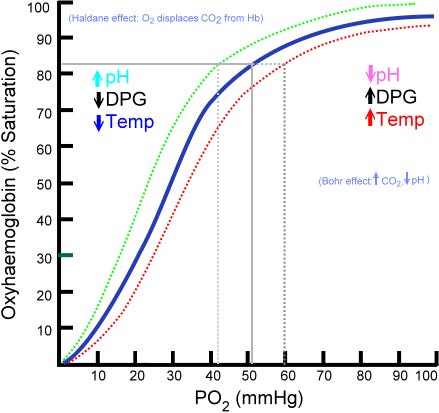
The Bohr Effect
“The Bohr effect refers to the shift in the oxygen dissociation curve caused by changes in the concentration of carbon dioxide or the pH of the environment… an increase in CO2 results in a decrease in blood pH, resulting in hemoglobin proteins releasing their load of oxygen.”
The vast majority of people have oxygen saturation levels between 96%-99% (using a standard pulse oximeter).
This is a measurement of the amount of oxygen-carrying hemoglobin in the blood relative to the amount of hemoglobin not carrying oxygen. In plain words, it shows us whether our blood is saturated with oxygen or not.
But that doesn’t mean that tissue oxygenation is normal.
According to the Bohr effect, it’s CO2, being an acidic oxide, that will decrease the affinity of hemoglobin for oxygen, allowing the latter to be released to the cells.
A lack of CO2 means lack of oxygen on a cellular level, even if you’re normoxic (i.e. normal oxygen saturation).
It’s this state of tissue hypoxia that causes disease.
“All chronic pain, suffering, and diseases are caused from a lack of oxygen at the cell level."
- Dr. Arthur C. Guyton, M.D., The Textbook of Medical Physiology
6) Increasing CO2
The desire to breathe is triggered by carbon dioxide, NOT lack of oxygen. Meaning that your central and peripheral chemoreceptors pick up changes in the blood pH and CSF, and signal the medulla oblongata to increase or decrease the respiratory rate (breathing frequency, tidal volume).
According to Dr. Buteyko, we’re over-breathing and expelling more CO2 than necessary. If we want to increase the amount of alveolar CO2 (amount of CO2 retained in the lungs) roughly speaking, without discomfort, we need to train in a way that normalizes our respiratory pattern. To do that, we need to create neurological and biochemical changes.
(There’s certainly enough evidence that people who are sick tend to have 2-3 times the minute ventilation of healthy adults)
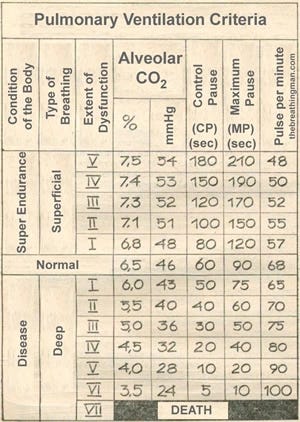
7) Control Pause Test
Dr Buteyko developed his method in order to get people from sick to healthy. In the process, he invented unique ways of measuring carbon dioxide levels and other vitals. The equipment was lost or confiscated after his laboratory was shut down.
But during that time, the Control Pause was developed as a DIY test to examine the condition of one’s health.
It is THE fundamental marker of progress. If your CP isn’t increasing, you aren’t doing Buteyko right.
The Control Pause test remains the most controversial instrument of the Buteyko method, due to the difficulty of performing it. It requires many attempts to get a “feel” for it and it fluctuates a lot throughout the day. Here’s how to perform it:
Sit for 5 minutes in a comfortable position, with your back straight, and your knees lower than your hips.
Then, after a random, normal, passive exhalation, hold your breath.
When the very first sensation of air hunger OR the desire to swallow OR a minor tremor in the diaphragm (whichever comes first), stop the test.
Your next inhalation should be identical to the inhalation before you began the test - easy and natural, without gasping for air. If it’s not, then you overdid it.
The breath hold time is your Control Pause score.
Your score in the morning, during the day, and evening will be different. That’s a feature not a bug, since the CP test takes a snapshot of your health at any given moment. There are parameters that naturally influence it (food, exercise, stress, etc) so obsessing over these minor ups and downs isn’t productive but you can glean valuable information about how your environment and habits affect your health.
What’s stable is your weekly average. Specifically, the weekly average of your morning Control Pause, measured less than 5 minutes upon waking up, in the position you’ve woken up.
According to Dr Buteyko, the score indicates the health of an individual better than any other measurement.
A (morning) Control Pause below 20s means: potential for disease
Between 20s and 30s: many symptoms begin to disappear
Between 30s and 40s: good health, medication is only needed for serious illnesses
Above 40s: near perfect health and high energy levels
Everyone is different of course, but I’ve found these milestones to be fairly accurate. Exceptions are to be expected. Keep in mind that a CP below 20s doesn’t mean you’re necessarily unhealthy, just that your body is more prone to an unhealthy state/it takes more to maintain your baseline.
“Life is suffering below 40s CP.”
- Dr Buteyko
If you’re wondering how CO2, breathing, and a random breath hold time test could determine your health, then you don’t understand how your cells and brain work. Let’s dive deeper into our physiology.
8) Cellular Respiration
Respiration is usually defined in the context of lungs, blood flow, and tissues. Yet, what happens on a large scale, happens on a small scale as well.
Have you considered why and how we use oxygen?
We need it to create energy = ATP (+ heat).
Cells are constantly respiring, using oxygen and expiring CO2.
This relationship between the two gases is the Respiratory Quotient:
RQ = CO2 eliminated / O2 consumed
The RQ determines how much oxygen is required and consumed to break down different macronutrients.
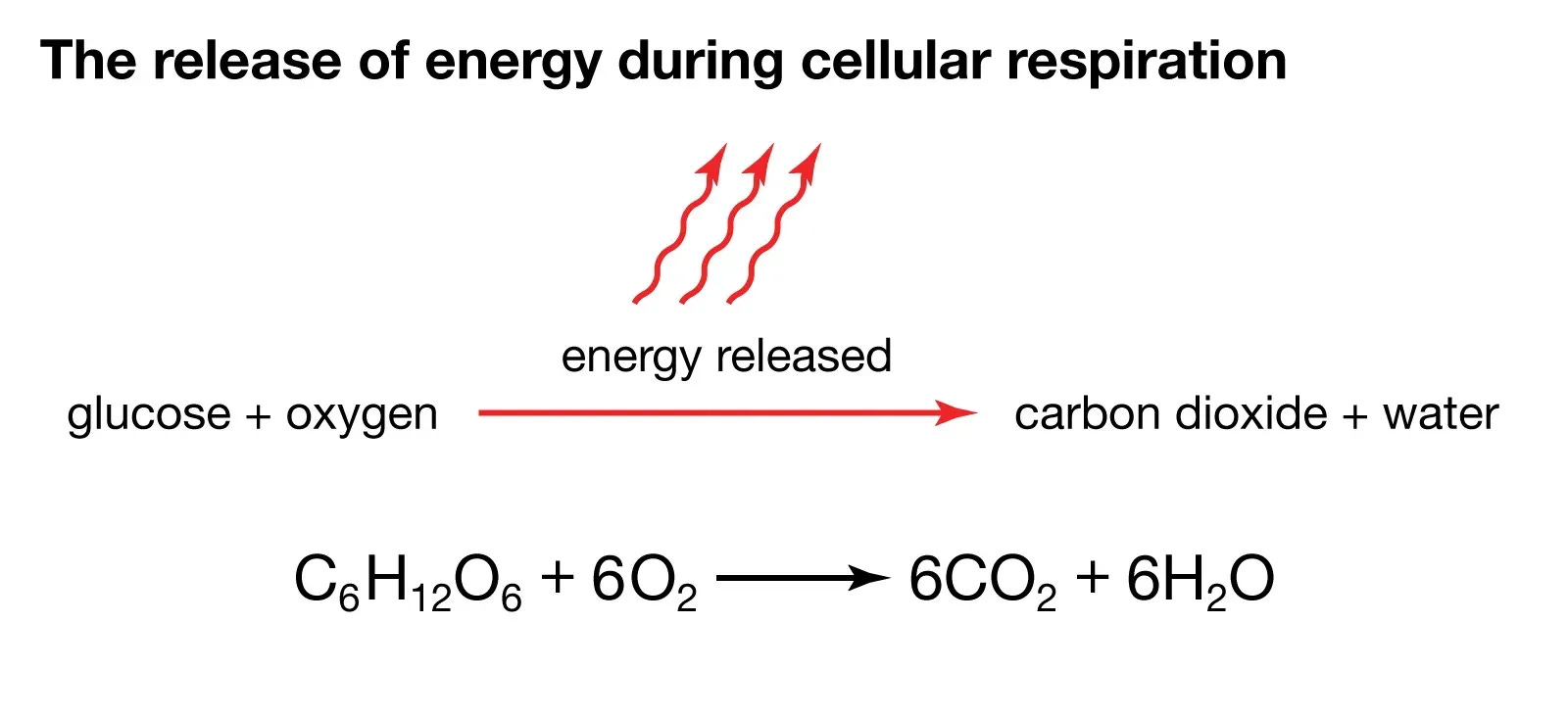
For glucose, the RQ = 1
C6H12O6 + 6 O2 → 6 CO2+ 6 H2O
6 molecules of oxygen are required for glucose (C6H12O6) and at the end of Krebs Cycle, you’ll have produced 6 molecules of CO2 and 6 molecules of water (H2O).
For fats, the RQ depends on the composition of the fatty acids but it’s roughly 0.7.
Given that most people end up using both glucose and fats, we estimate that the average RQ is about 0.8.
But how is all that relevant?
It’s important to look at biological systems holistically, accounting for all their dynamic, moving parts.
Cellular metabolism, the very process that produces our energy in ATP form, is dependent on ~3 different steps:
Glycolysis
The Krebs Cycle
Oxidative Phosphorylation/Electron Transport Chain
The first step, glycolysis, doesn’t require oxygen and can happen anaerobically, using NAD+ as the oxidative agent.
(The remaining steps do require oxygen. In fact, the final electron acceptor in the last stage of the electron transport chain is oxygen)
When oxygen isn’t available, we’re stuck in glycolysis. Since we have a limited pool of NAD+, pyruvate is reduced to lactate while NADH is oxidized to regenerate NAD+. This is called fermentation, the “lactic acid” metabolism (quick note: the human body doesn’t actually produce lactic acid - nor ferment -, just lactate and H+ but for the sake of quick communication, we’ll stick with these terms)
Cellular respiration yields 18 times more ATP per glucose molecule than fermentation.
When this continues to happen chronically (tissue hypoxia), we enter a vicious circle where not only we aren’t producing enough energy and deplete NAD, the amount of CO2 we produce (from the Krebs Cycle) is diminished.
And if you remember the Bohr effect, that means O2 isn’t optimally delivered to the tissues and we continue producing lactic acid - even at rest.
Lactic acid in turn displaces both O2 and CO2. And the cycle continues.
CO2 is necessary to ensure oxygen is available during cellular respiration.
And it all starts with normalizing your breathing.
Lactate
Everyone is producing lactate and H+ at rest. Without it, you’d be dead. But if you’re chronically stressed, you’re more likely to produce abnormal levels in abnormal conditions.
Lactate and H+ increase your respiratory drive but since you can’t exhale lactate, you’ll exhale CO2 instead. Can you see how that can be problematic? You’re in a state of pseudohypoxia, as your breathing appears “normal” but you’re, in fact, hyperventilating.
Long term, you’re reducing CO2 and consequently the oxygen available for your cells. On top of that, there’s a chance that you’re reducing chemosensitivity (your chemoreceptors don’t pick up changes in pH or CO2 content), creating an acid-base imbalance and making it harder to normalize your breathing.
9) Neurological Factors that Influence Breathing
Contrary to what most will tell you, respiration is still somewhat of a mystery.
Given that breathing is the beginning and the end of metabolism, it’s subject to a dizzying number of parameters that make it particularly hard to separate the layers of causation.
In the last 30 or so years, we’ve discovered that the Pre-Bötzinger complex is responsible for establishing rhythmogenesis (the rhythm of inhalation and exhalation; breathing pattern) in the brain.
The phrenic nerve provides motor supply to the diaphragm.
There are mechanoreceptors, long reflexes like the hering-breuer, and stretch receptors that control the expansion of the thorax, the inflation and deflation of the lungs, etc.
Even recently (less than a decade ago) we identified the retrotrapezoid nucleus as a major part of the medulla's respiratory control center that influences the preBötC.
On a practical level, CO2 above your baseline is largely anxiogenic so we tend to confuse the acute reaction during exposure with the long-term adaptation. CO2 happens to be the strongest vasodilator, smooth muscle relaxant, and in general very positive for the robustness of your nervous system.
There are always new discoveries that challenge the dominant carboxy-centric explanation of respiration. But the reason we focus on CO2 is because CO2 happens to be present in or influencing all of the above.
The following are just a few examples.
10) CO2 is the chief (para)hormone of the body
A parahormone acts like a hormone but is a product of the normal metabolism of cells.
"Carbon dioxide is the chief [para]hormone of the entire body; it is the only one that is produced by every tissue and that probably acts on every organ."
Indeed, carbon dioxide is a byproduct of cellular metabolism that acts on every part of your body:
1) It regulates pH through its conversion to bicarbonate-/-carbonic acid
2) Monitors respiration via influencing chemoreceptors through their sensing of H+ in the CSF
3) CO2 promotes vasodilation and influences baroreception, regulating blood pressure and cardiac output
4) Influences gene expression (example; "Recent advances have identified the repression of the NFκB transcriptional pathway by CO2 in a manner which may be of therapeutic benefit in chronic inflammatory disease.")
5) Following from #4, it plays a role in inflammation (example; enhanced anti-inflammatory cytokine production/IL-10, angiogenesis)
6) Cont. Inhibits MAPK signaling pathways: "The benefits of using elevated CO2 levels in the treatment of various diseases are reflected in numerous completed and ongoing clinical trials established to evaluate CO2 use as a medication. Advances in research on the regulation of CO2-MAPK may significantly increase the number of new therapeutic applications of CO2."
7) CO2 can even regulate cholesterol via SREBP-2 -> High SREBP-2 expression is associated with hypercholesterolemia.
8) CO2 affects cerebral blood flow severely. Under a certain CO2 threshold, CBS is increased without changes in blood pressure.
9) In this way, CO2 is a primary instigator of nervous system shifts and autoregulation (sympathetic/para)
10) The Bohr effect described by oxygen dissociation curves is dependent on CO2/PCO2 (the Bohr effect shows the affinity of hemoglobin for oxygen - how easy it is for them to release their oxygen load to the cells)
11) CO2 is an inhibitor of ROS generation by cells. The build-up of ROS in the cells can cause damage to DNA, RNA, and proteins.
12) It enhances feedback from stretch receptors and reflexes —increased stimulation of motor neurons that control the muscles of respiration, including the diaphragm and intercostal muscles (see phrenic nerve)
13) Cranial nerves are influenced by changes in respiration (CO2 causes changes in the sensitivity of the vagus nerve nuclei, for example. The glossopharyngeal nerve is involved in transmitting signals related to the regulation of respiration and swallowing)
14) CO2 prevents the degranulation of mast cells (allergies, inflammation)
15) A slightly acidic environment seems to promote isotope discrimination, allowing the faster turnover of light hydrogen as opposed to the heavier deuterium.
As you can see, separating the normal functioning of an organism from the presence of CO2 is impossible.
11) Normal Respiration
Your respiratory rate is breathing frequency (how many breaths per minute) and tidal volume (L of air per inhalation/exhalation). You can have a low BF and a high tidal volume, and vice versa. Both are considered “hyperventilation”.
Normal breathing frequency is 6 to 10 bpm (yes, in contrast to what textbooks claim today)
We breathe using the diaphragm and intercostal muscles (secondary respiratory muscles like the chest, scalenes, sternocliedomastoid, traps, etc are used during exercise but a sign of distress if engaged at rest)
The inhalations are always shorter than the exhalations. Exhalations are passive and last longer than inhalations. Exhalations are caused by the elastic recoil of the lung tissue, followed by the simultaneous relaxation of the respiratory muscles.
There’s a natural pause after an exhalation that can last between 4 to 10 seconds. There’s a half a second pause after the inhalation. Inhalations are short, between 1 to 1.5 seconds.
Nose breathing 24/7 is the norm, with the exception of very hard physical exercise.
Normal breathing is easy, soft, quiet, natural, deep, and anchored.
12) General Guidelines for Breathing
According to Dr Buteyko, you should:
Nose breathe 24/7.
Tape your mouth at night if you need to.
Keep an upright posture (important to not collapse your chest).
Exercise/move for 3-4 hours every day (imo, you should exercise as much as possible but stop right before it stops being energizing).
Stand more than you sit. Sit on the floor, rather than a chair when possible
Spend as much time as possible outside.
There’s more you can do but I’m focusing on what Dr Buteyko said.
13) How to Practice the Buteyko Method
As I’ve mentioned in #4, there are many exercises that can work as long as they adhere to the basic principles.
The following are easy and simple to perform but depending on your motivation, they can get you far enough.
Exercise A
Sit in a comfortable position with your back straight, and your knees lower than your hips.
Breathe normally for 2 minutes and let everything settle.
Then, bring your attention to the (natural) pause after an exhalation ends and before the next inhalation begins.
Slowly start elongating these gaps until you feel mild to moderate air hunger.
Maintain the air hunger for 15 to 20 minutes, while staying relaxed through the discomfort (equanimity).
You must breathe using your diaphragm. Remember that your exhalations must be passive.
Figuring the right pace and degree of air hunger is a skill. If you do it right, you’ll feel hot and sweat.
Alternative: Instead of elongating the pause after the exhalation, focus on reducing the volume of your inhalations. Some people find it easier to maintain air hunger by reducing their inhalations to 80% to 90% (of the air you breathe in during a normal inhalation).
Find the sweet spot so that you can experience the discomfort without triggering a big sympathetic response:
The secret to an effective Buteyko session is to ride the sensation of air hunger at the edge of panic without letting it consume you to the point of eliciting an uncontrollable reaction.
Eventually, after many weeks of daily practice, you’ll find that the sensation of air hunger relaxes you(!!)
Exercise B
Start walking
After a normal exhalation, pinch your nose and count 5 steps
Release and breathe normally
Once the air hunger subsides, repeat and do 5+5 (10) steps
Continue
Add 5 steps every cycle, until you hit 50 steps or 12 minutes pass. Whichever comes first.
If you can’t add 5 steps or the air hunger is too much, repeat the previous number of steps.
Once you hit 20+ steps, you can take longer breaks, 1-2 minutes, instead of going by feel. It’s up to you.
Here’s what a session should look like:
1st cycle: 5 steps, 15s until the air hunger subsided
2nd cycle: 10 steps, 30s until the air hunger subsided
3rd cycle: 15 steps, 40s until the air hunger subsided
4th cycle: 19 steps, air hunger too strong
5th cycle: 15 steps, 1 minute
6th cycle: 20 steps, 2 minutes
7th cycle: 25 steps, 30s
.
.
.
.
11th cycle: 50 steps, end the session
Once you can hit 50 steps comfortably in every session, work toward reducing the recovery time or hit 50 steps twice in one session, or many times back to back.
This is grunt work, for the most part. A little autoregulation is necessary but you don’t have to think too much. Just do your sessions and push yourself until it becomes intense (use strong/very strong air hunger sparingly).
A successful session means that your control pause will 2s-5s afterward. Wait 5 minutes after a seated session and 10-15 minutes after a walking session before measuring your CP.
If you’re unsuccessful, a) weren’t relaxed enough b) didn’t feel air hunger consistently c) many other reasons but depend on the individual.
You should be doing 3-4 sessions every day (~1 hour)
Leave 2 hours between each session.
Not directly after eating - relatively empty stomach.
Discuss with your doctor before engaging in this kind of practice. It isn’t a relaxing, kumbaya, 10 minutes breathwork technique. You must be careful, especially if you have a serious health condition.
12) Link to Esoteric Practices
It’s obvious that Dr Buteyko was interested in more than just the physical effects. In fact, in his Moscow lecture he mentioned yoga over 20 times and he doesn’t shy away from admitting that his method most likely existed already in eastern practices.
Sophisticated breathing exercises have been around for thousands of years. The retention of breath as described in Kumbhaka pranayama or the physical sensation of piti, or the formation of the energetic center of the Xiantian from the Taoist tradition comes very close to some of the experiences of Buteyko’s students.
(My recommendations don’t extend beyond learning to apply Buteyko. Everyone has their own take on health and life - I don’t agree with everything they say nor am I affiliated with them)
1) Look into the Frolov machine if you’re someone who prefers a more direct, mechanical approach to breathwork. Long-term, the breathing techniques will prove more effective but some people report better luck with Frolov in the beginning (remember, it’s about increasing your CP score)
I’ll eventually write a short manual on how to use it but for now, rely on the instructions that come with it.
If possible, find a DINAMIKA one.
2) Similarly, CarboHaler for administrating carbogen (a mixture of oxygen and carbon dioxide). I don’t believe it’s a free lunch, because I find that you still need to apply Buteyko’s principles (i.e., to experience air hunger) to get long-term benefits, but it could be used to enhance your sessions or make them a little easier to control.
I wouldn’t go above a 3%-5% mixture and I’d CERTAINLY TALK TO MY DOCTOR before using it.
Disclaimer: I haven’t used this company’s product. I’m not affiliated with them. Their product seems to do what it’s supposed to do so there! Less expensive options are rarely up to par.
FAQ
1) “But elevated CO2 in small spaces has been shown to cause cognitive issues.”
This is almost true. As I’ve mentioned, CO2 increases respiratory drive and can cause a mild sympathetic nervous system shift. But when you’re adapted to a higher CO2 baseline, you won’t experience this effect.
In many cases, CO2 is an indicator of the accumulation of bioeffluents, lack of negative ions, and poor air quality in general.
Studies like this show that administrating CO2 in a controlled environment doesn’t have the same effects.
2) “CO2 increases respiratory drive. If you’re breathing less, doesn’t that mean that you have low CO2?”
See #8, under Lactate. It’s not only CO2 that stimulates breathing.
3) “If you breathe less, does that mean you’re getting less oxygen in your body?”
Not in normal conditions. The inspired air is roughly 21% oxygen and the air we exhale is 17% oxygen, meaning we only utilize 4%-5% of oxygen. What’s important is that the lung’s ventilation-perfusion is healthy and the transfer of oxygen from the blood to the tissues is happening optimally. Oxygen availability isn’t an issue, delivery is.
There you have it. Hopefully, this is helpful to some of you or at least gives you a better understanding of what the “mystical” and convoluted Buteyko method actually is.
On a personal note, I believe everyone should spend at least a year trying to increase their control pause to the absolute maximum their time, genetics, and motivation allow - even if you don’t get the supraphysiological benefits, you’ll get some and you’ll certainly learn many things about your own body and how it’s affected by your breath and nervous system.
Buteyko actualizes the human potential. Don’t miss out :)
Hyde, thanks for a fantastic article. I've been practicing pranayama for about six months and this inspired me to experiment with switching to Buteyko's method.
One question - in section 13, you say "A successful session means that your control pause will 2s-5s afterward." Did you mean will shorten by (or lengthen by) 2s-5s? And is that immediately or after the recommended 5-15 minute period before measuring?
















Hyde, thanks for a fantastic article. I've been practicing pranayama for about six months and this inspired me to experiment with switching to Buteyko's method.
One question - in section 13, you say "A successful session means that your control pause will 2s-5s afterward." Did you mean will shorten by (or lengthen by) 2s-5s? And is that immediately or after the recommended 5-15 minute period before measuring?
I know this can be annoying because is the most asi question but I haven’t found a reference of this in the comments of other posts.
I haven’t found chronic sinusitis, for a couple of years already. What’s the best way to improve? 🙏🏻