



Against Fear; exploration of its biological manifestation
The effects of CO2 and hyperventilation on panic, anxiety, and stress

It’s obvious that hyperventilation (HV) is one of the hallmarks of panic. Simply put, the body increases your respiratory rate because it anticipates danger so it prepares to fight or flight and exert more effort. The adrenergic system is engaged and there’s a shift in sympathetic nervous system dominance.
This is well-understood and empirically validated. But what if HV itself was causative of panic and other similar disorders? Indeed, hyperventilation is far more insidious and chronic.
Primary hyperventilation syndrome is found in ~10% of the gen pop, with concerns that this is just the tip of the iceberg due to diagnostic criteria.

The intermittent nature of breathing and the myriad of buffer mechanisms that can compensate making it hard to pin down and differentiate HVS (hyperventilation syndrome). But let’s look at some of the physiological symptoms:
“The breathing pattern of these patients were typically described as disorganized, with lower than normal PCO2 levels, rapid respiration rates, frequent sighing, and predominately thoracic rather than abdominal breathing.”
I speak from experience when I say that a significant minority of the population has exhibited these symptoms in the last 7 days. And while hyperventilation and HSV are somewhat different, the former is a less severe but much more frequent manifestation with subtle yet noticeable symptomatology.
Is this enough to suggest that a dysfunctional breathing pattern could be a cofactor in panic attacks, GAD, and even chronic fatigue?
Maybe…
The Underlying Mechanism(s)
Hyperventilation is defined by Guyton as the “irregular breathing that occurs when the rate or tidal volume of breathing eliminates more carbon dioxide than the body can produce.”
It’s normal to breathe more when exertion is expected but when “danger” or necessity isn’t present, excessive breathing results in hypocapnia (less CO2). Because of the way rhythmogenesis1 and our nervous system work, over time this reaction can alter our reflexive breathing pattern. Taking it to the extreme, it can result in suffocation of our energy production; simply put, hypocapnia impairs the Bohr effect so the transfer of oxygen from the blood to the tissues becomes suboptimal, also causing the production of excess lactate and H+ at rest, which will further intensify the positive feedback loop.
On that basis alone, you can see how vital it is to take control of your breathing. Yet, it doesn’t stop here.
Cerebral Blood Flow
Hypocapnia is vasoconstrictive:
Lower PCO2 causes blood vessels to constrict reducing blood flow to the brain.
This is why HV, which reduces CO2 levels, leads to decreased cerebral blood flow.
For every 1 torr (=1mmHG) change in PCO2, cerebral blood flow changes by 1 to 2 ml/min per 100 grams of brain tissue.
This means that a small change in CO2 levels can significantly affect how much blood the brain receives (Hyperventilation and Cerebral Blood Flow)
Can we draw a causative link? Yes we can:
“Subjects with severe anxiety showed least hypercarbic CBF increase (indicating cerebral vasoconstriction) and maximal increase in forehead skin perfusion. Those with minimal anxiety had most hypercarbic cerebral vasodilation and least increase in forehead skin perfusion.” (Intracranial and extracranial blood flow during acute anxiety)
This is the reason low-level anticipatory anxiety can feel like it’s making you dumber. You’re quite literally suffocating your brain.
But why do we hyperventilate to begin with? Well, one potential factor, especially in the context of our investigation, is that we’re oversensitive to changes in CO2. It’s possible that we aren’t hyperventilating only because of panic or GAD but hyperventilation itself and CO2 above baseline could cause the symptoms.
Sensitivity to CO2 = Manifestation of Fear?
One way to research “fear” and how it affects our behavior, cognition, etc is through CO2 challenges.
Inhalation of 35% CO2 caused panic in ALL subjects, regardless of their (panic disorder, social inhibition, control group) diagnosis.


This Gorman paper conclusively establishes that CO2 alone can cause panic2. Previous research showcased a greater ventilatory response in panic disorder patients, making the point that the feeling of suffocation could be memory-related to panic attacks. Indeed, hyperventilation itself can trigger panic but CO2 is more anxiogenic (see comparison between room air hyperventilation vs 5%/7% CO2 inhalation)
In practice, what that tells us is that there’s a mechanism that involves a direct interaction between carbon dioxide and fear centers. CO2 activates a fear network involving the amygdala and prefrontal cortex, promoting vigilance to environmental threats and impairing top-down regulation of attention. Participants made more errors orienting toward negative stimuli during antisaccade trials with CO2 than with air.
Moreso, changes in connectivity between the amygdala and the dorsal periaqueductal gray in PTSD are observed, with the PAG modulating the hypercapnic ventilatory response.
Here’s where we are:
Hyperventilation is bad and can cause stress and impaired cognitive function
Sensitivity to CO2 is bad and can cause stress and impaired cognitive function3
If you hyperventilate to expel CO2, long term you’ll suffer
The interesting thing about the mind-body is that it’s really just one. We often make the mistake of observing cause and effect manifesting in two different sides (cause in the body and effect in the mind or vice versa) but in reality, the effect becomes the cause, as if to retroactively enable the cause.
One simple example is the common, reflexive pattern of holding your breath when you’re hyperfocused.
GABA, Overstimulation, and Equanimity
Even now reading this, you’re likely holding your breath, tensing your abdomen, or inhaling high up in your chest. Maybe you’re mouth breathing! Whether the cause is bad posture or low-level agitation due to exertion, using secondary respiratory muscles is indicative of stress and stress is mediated by an overexcited nervous system. The latter will manifest the very symptoms that are also the cause (e.g. are you hunched over because you’re stressed or you’re stressed because you’re hunched over, are you overbreathing because you’re stressed or you’re stressed because you’re overbreathing…)
One way your body instigates and deals with the stimulation is through the GABA-glutamate effect on the brain.
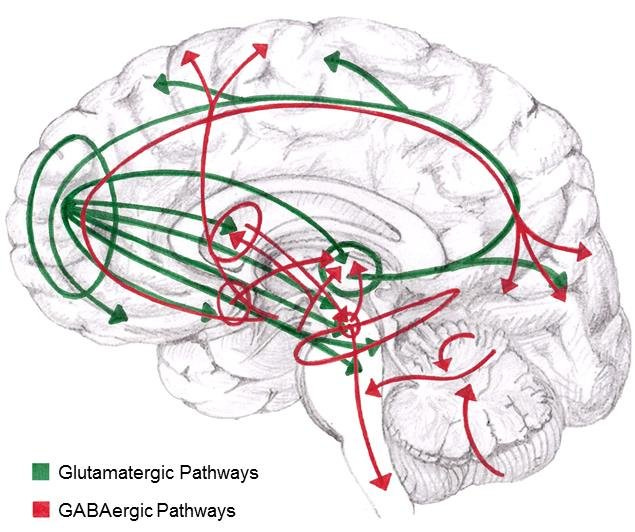
I’m sure you’re familiar with some of the touted benefits of GABA but my approach is more neutral. Think of glutamate as GREEN → GO and GABA as RED → STOP in the context of nerve cell to nerve cell communication. Green excites, Red inhibits.
When stimulus enters the brain, in our case CO2, then there’s subsequent glutamatergic activity, to facilitate processing:
“Increased activity in emotion-processing brain regions in patients who have an anxiety disorder could result from decreased inhibitory signaling by γ-amino-butyric-acid (GABA) or increased excitatory neurotransmission by glutamate.”
GABA, being in a sense neuroprotective, inhibits this reaction calming overactive neural circuits. This is a natural give and take that maintains equilibrium in the brain.
Panic and anxiety are the imbalance of this interaction, and per the previous sections of the essay, link GABA-CO2-respiration together4.
Blissful States
In the 1920s, Dr Ladislas Meduna developed the Meduna mixture, a gas comprised of (originally) 30% carbon dioxide and 70% oxygen. Today, we use carbogen to facilitate better ventilation in a clinical setting (also therapeutically DIY) but back then Meduna had far more ambitious goals.
If you remember, the 30/70 admixture produces potent panic in ALL subjects. It’s liquid panic, for lack of better words. Well, Meduna noticed that his gas, even though it did cause the intense feeling of suffocation, it also generated profound, altered states:
From “Carbon Dioxide Therapy. A Neurophysiological Treatment of Nervous Disorders”:
“…and I pressed close the warmth and tender strength and felt assurance of enough power to overcome whatever lay ahead for me as a human being.”
“Reached a greater Spirit with Whom there was a communion, producing a remarkable, new relaxation and deep security. Through this communion I seemed to receive assurance that the petite problems or whatever was bothering the human being that was me huddled down on the earth, would work out all right and that I had no need to worry.”
“It was a wonderful feeling. It was marvelous. I felt very light… And then it felt as if there were a space of time when I knew something had happened to me and I wasn’t sure what it was. And then I felt a wonderful feeling as if I was out in space.”
I hope you don’t try this at home. It’s a very bad idea since many subjects passed out or had convulsions.
A more recent study found that “Higher initial petCO2 and higher arterial blood pCO2 proved to be important in the provoking of Near Death Experiences.” There’s obviously something psychoactive that gets triggered in the presence of CO2.
But the main takeaway is that there’s a targeted response in the brain that offsets the induced panic. While in Meduna’s experiments the response was to shut down, it highlighted that there’s an inhibitory reaction to CO2 after exposure.
GABA-dopamine mediated(?)
I’ve given instructions for the Buteyko method to thousands of people at this point. For those of you who are unfamiliar, read this first (tl;dr we use air hunger from CO2 to normalize our breathing pattern by taking advantage of the CO2→pH→chemoreceptors→brainstem connection).
The main feedback I receive is that originally the breathholds felt suffocating and induced panic but after training to maintain equanimity under stress, the breathholds started feeling relaxing and even euphoric at the point of initiation and until the levels of CO2 climbed beyond one’s comfortable baseline.
This is evidence that we can indeed retrain the way we react to what is, fundamentally, the key ingredient to panic, anxiety, and social phobia.
One of the mechanisms of actions (imo) is a combination of GABA-ergic activity and dopaminergic activity in the ventral tegmental area. While these two have an antagonistic relationship, their interactions give rise to a stable, pleasant state.

When exposed to “unpleasant” stimuli, there’s an uptick in GABA neurons and a decrease in dopamine neurons. At the same time, overexcitation of dopamine neurons while suppressing GABA receptors results in mania and panic. During a Buteyko session, we ride the edge between panic and relaxation, “relearning” the neurological response to elevated CO2 levels.
Excitement is anxiety sans fear
Another way GABA directly controls the ventilatory response due to panic/hyperventilation/CO2, protecting the brain from hypoxia and respiratory alkalosis, is through its effect on the preBötzinger complex.
GABA enhances the inhibitory activity in the preBötC5, ensuring that the inspiratory and post-inspiratory phase is smooth and continuous. It halts hyperventilation and provides the necessary “calming” effects (sighs, gasps, large tidal volume represent a paradoxical breathing pattern, which includes an inhibition blockade)
There’s some evidence that CO2 directly modulates GABA-A receptors in animal model studies. The way GABA provides tonic inhibition, though, might be more indirect:
“1 min of 35% CO(2)/65% air produced anxiogenic effects in a rat model of anxiety, to a similar extent to the anxiogenic betacarboline derivative FG7142, The effects of both anxiogenic stimuli were abolished with pre-treatment with alprazolam (0.5 mg/kg), but only those of FG7142, not CO(2), was blocked by a benzodiazepine antagonist.”
FG7142 acts on benzodiazepine receptors, and its anxiogenic effects can be blocked by a benzodiazepine receptor antagonist.
CO2-induced anxiety doesn't depend on benzodiazepine receptors.
This means that flumazenil doesn't block CO2-induced anxiety because CO2-induced anxiety is not mediated by the same receptor mechanism, however benzodiazepines like alprazolam can help reduce this anxiety by potentiating GABA activity, which helps counterbalance the excitatory signals that contribute to stress.
(Not a) Conclusion
One of the key ways to expand your comfort zone is by doing hard things as if they aren’t hard.
Your mental and physical response to stress and challenges can trigger very real biochemical changes that “reset” and influence the baseline state of your physiology.
While all of this is basically a crude hypothesis, I believe that it points in the right direction. The way our inhibitory and excitatory pathways work synergistically gives rise to the potential for transformation. Basically, you can’t think your way out of your current self but you can certainly expose yourself, willingly, to the conditions that can change you on a fundamental level.
During a Buteyko session, when the air hunger goes from anxiety-inducing to bliss, there’s a distinct feeling of flow and perfect mental clarity. We are, in real time, reconfiguring the way anxiety and stress manifest and affect the body. From punishment to reward.
It’s up to you, reader, to make your own conclusions about the nature of fear, stress, and CO2.
Chemoreceptors sense changes in the blood pH and increase/decrease the respiratory rate to maintain the acid-base balance. The medulla oblongata, the respiratory center, as well as the preBötzinger complex, accommodate by sending inhibitory or excitatory signals, slowly “resetting” the basic, reflexive breathing pattern.
Sleep apnea, that causes elevated CO2 levels, is one the primary culprits for sleep paralysis
Fear is the mind killer
I won’t talk about HRV, vagal tone, etc. Even though they certainly play an important role, they’d expand the scope of the essay beyond its purpose.
Inhibitory doesn't mean lower respiratory rate necessarily. What's inhibited is the post-inspiratory phase, i.e. it's cut short so the passive exhalation can begin (relatively) faster. But at the same time that also doesn't mean a higher respiratory rate either. It's the transition, in all phases of respiration, that becomes smoother.